Pacemakers are primarily implanted under local anesthesia. Sedation is supplemental and enhances patient comfort and operational safety.

If proper local anesthesia is given, the vascular access steps should be painless – however in practice most patients (especially the young adults) are extremely anxious and deep tissue local anaesthesia is not always perfect – therefore there is always a chance that a patient might react violently even to a minimally painful stimulus posing a danger to himself and the operators. It is paramount that patients do not move or react violently to minimal pain during vascular access as this may lead to a pneumothorax by accidental puncture. Therefore sedation helps in enhancing operational safety and increases patient comfort.
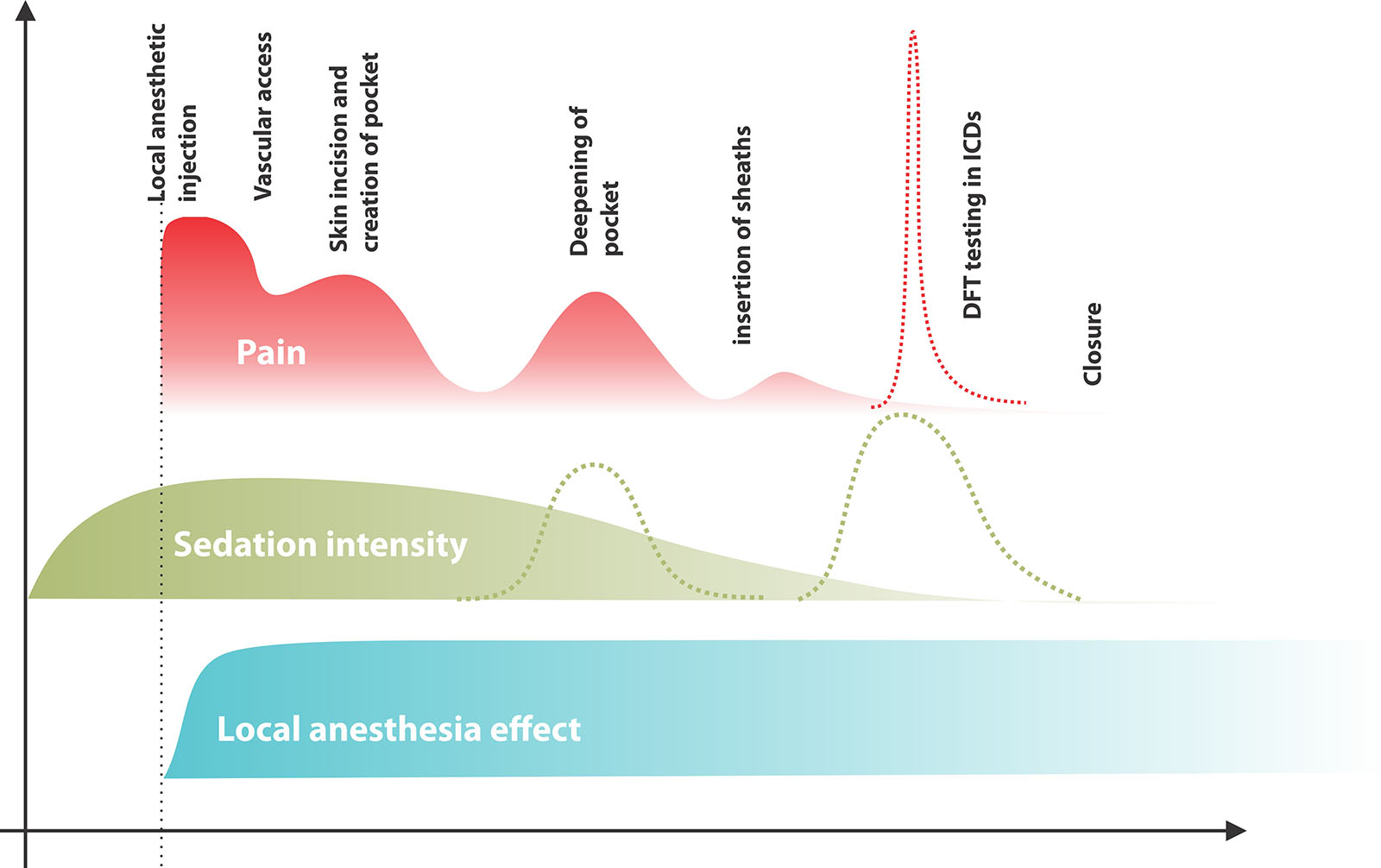
Figure : Principle sources of pain and sedation cascade. Most patients can complete the procedure with a single administration of sedatives at the beginning followed by local anaesthesia. Additional doses of sedatives are require if the pocket has to be made very large (e.g. ICD) or during defibrillation testing in ICDs (additional top ups are in green dashes)
Out of the above, ICD DFT testing cannot be mitigated with local anesthetics and need good sedation. The other steps can be managed with a combination of LA and Sedation.
Caution must be exercised in elderly and in situations where there is no dedicated anesthetist available for procedural sedation. The topic of procedural sedation (so called with a confusing term “conscious sedation”) is out of the scope of this discussion and readers are requested to read up on their own [Note: there are strict guidelines on procedural sedation which vary from jurisdiction – and the primary operator assumes all responsibility of knowing these guidelines before sedation is used] – the practice that is described below is an outline only.
Our workflow for sedation
Briefly our technique of sedation is as follows – (we do not have a dedicated anesthesia specialist at bedside, but on call cardiac surgery anesthetist can be summoned to theater within 10-15 minutes in case of emergency) [Note: All pediatric and potentially uncooperative teenagers are done under GA with a dedicated anesthetist in attendance] For safe and efficient sedation, the following personnel and items and must be present in the theater in addition to the standard equipment necessary for safe pacing:
- A physician capable of cardiopulmonary resuscitation in addition to the implanter – in our case it’s usually another EP fellow or EP duty medical officer.
- At dedicated nurse to prepare and administer medications (this nurse is always present in the theater)
- For potentially problematic patients an additional easily accessible separate intravenous cannula on the opposite hand to the side of operation.
- Working pulse oximeter with waveform and heart rate in addition to SpO2 display
- Ample supply of wall oxygen and a backup cylinder based oxygen supply in theatre
- Fully equipped emergency crash cart with airway equipment
- Fully functional suction apparatus and necessary tubes
- Full and additional doses of flumenazil and naloxone in addition to standard cardio-pulmonary resuscitation medications
We use a combination of morphine and midazolam for sedation. In cases where short acting deep sedation is needed rapidly we also use fentanyl. Although theoretical respiratory depressive effect of morphine is more, we prefer morphine as analgesic instead of fentanyl for all routine cases because,
- Morphine action is relatively long lasting (although the onset is slow) which can cover the procedure
- Staff experience with morphine is much more than with fentanyl
- Anxiolytic effect of morphine is greater than of fentanyl (whereas fentanyl “knocks off the patient” for a shorter period)
- Morphine is readily available at a lesser cost
In specific instances, we do use fentanyl – example would be – a highly sensitive patient who poses a danger to him by struggling even on mild pain. Here we would initiate the procedure with fentanyl where a short acting deep sedation would ensure facilitating safe vascular access.
The role of midazolam is sedation and amnesic effect. Even if the procedure “appeared” uncomfortable to the patient, vast majority of them barely remember the procedure if adequate amount of midazolam is given. This is an important benefit of benzodiazepines as certain patients may be undergoing repeated procedures (e.g. box changes, lead re-position etc.) It is also a critical medication that we administer during defbrillation threshold testing of ICDs to ensure patient comfort and amnesia of the DFT procedure.
Sedative drugs along with an anti-emetic are administered before the cleaning of torso is commenced. This is necessary as standard morphine and midazolam take about 10 minutes for their full action. [If fentanyl is used, it is injected just before the local anesthetic is given to the operative site]. If the IV cannula is on the ipsilateral side (e.g. because of venography need) – an extension tube is used to administer medications – rather than directly accessing the cannula. Directly accessing the cannula will bring un-sterile personnel near the sterile field and increase the risk of infection
An important caveat of using midazolam is the risk of paradoxical behavior (restless and agitation) in elderly patients. Combined with other risks of sedation, we avoid sedatives altogether and try to do the procedure with local anaesthesia alone.
Personal experience suggests that elderly patients tolerate the procedure very well without sedatives provided the initial local anaesthesia is given meticulously and carefully. Author’s described technique for local anaestheisa is culmination of that quest to do the procedure only with local anaesthesia.
For the occasional highly anxious elderly patient, we may give a small dose of opiod (e.g. morphine 1 mg) for purely anxiolysis. We have also observed that pre-treatment with an opioid makes the chance of a benzodiazepine induced aggressive behavior much less and if there is a need for a benzodiazepine, it is given after the opiod injection. In any case the total doses are kept to a minimum. Regardless, the threshold to summon an anesthetist should be low when dealing with elderly patients – because elderly patients have poor cardiovascular reserve and a sedation mishap may rapidly become fatal.
Morphine and midazolam are diluted to 1 mg/ in 1 ml concentration and pre-loaded to 10 ml syringes for safe and controlled injection. None of the drugs are injected in their native concentrations. In addition to the sedatives, adrenaline (10ml of 1:10,000 solution) atropine (1.2 mg in 10 ml) is also drawn up to labelled syringes and kept in the medication tray – to be used in case of emergency. Our preferred anti-emetic is ondensetron (4 mg stat dose) but is not frequently available and therefore we resort to IV metoclopramide. So far we have not experienced a dystonic reaction to metoclopramide in adults. (However caution must be taken in patients with QT prolongation. In such cases, first midazolam is given and after the onset of sedation, morphine or fentanyl is given. The benzodiazepine itself has mild anti-emetic properties and we avoid metoclopramide) Good theater practice dictate that all medications are in syringes which have been properly labeled before bought near the table.
Figure : Drug box. All essential drugs are in kept in this easily accessible box.
Figure : All drugs that are used /potentially needed are drawn onto labelled syringes. Preparation of these syringes should be done by the nurse who stays with the procedure and administers the drugs.
Figure : Pulse oximeter with waveform. The pulse oximeter with waveform display and pulse counter serves two purposes – First, it keeps track of saturation. Secondly, it gives idea of the effective perfusing rhythm. This second feature is very valuable to assess active rhythm when there is a discrepancy in the ECG monitor. A good perfusing waveform on the pulse oximeter indicates the rhythm has to be good at that point (i.e. for example in a TPM dependent patient, the TPM is indeed capturing)
Soon as IV cannulation is established, 1 ml of the diluted antibiotic is given and observed for one minute and the remainder of the antibiotic is injected. See here for antibiotic prophylaxis. Thereafter the anti-emetic is given followed by Midazolam for sedation which is given in aliquots of 1.5 – 2.5 mg. This is supplemented by morphine for analgesia in aliquots of 1.5 – 3.0 mg. If fentanyl is used, the vast majority can be sedated adequately with a single dose of 50 micrograms (in addition to midazolam) but occasionally one may need 75 t0 100 micrograms.
Practical tip : Observe the patient’s reaction to pain during IV cannulation : A remarkable tolerance to the procedure indicates that the patient has high pain threshold and your strategy should be to minimize sedative use and optimize local anaesthesia. An opposite reaction (exaggerated pain response) indicates that strong sedation may be required at least for the initial steps.
Now, oxygen by a face mask or nasal cannula is attached and the patient is prepped up for the surgery. For sedated patients, oxygen supplementation is a must. However if no sedation was used – the mask / prongs may be uncomfortable for the patient and routine oxygen administration is unnecessary. In COPD patients, oxygen supplementation must be carefully adjusted to maintain a reasonable saturation for the given patient – not to aim for >95%
Continuous pulse oximetry is used for monitoring saturation. Personal experience suggests the first dose of midazolam and opiod is adequate for most patients to complete the surgery when local anesthesia is established properly. Additional top-up doses of sedatives are required when the procedure is complex (ICD, CRT) or if the patient is extremely anxious or pain sensitive. A note of caution applies to elderly patients. These patients can paradoxically get agitated to benzodiazepines and also easily develop respiratory depression by over sedation. Our practice is to give the opiod only and pay meticulous attention to local anaesthesia [ see red box above and here for pacing in elderly].
Tips to success are –
- Good theatre protocol and not taking shortcuts
- All personnel knowing the advantages, limitations and dangers of sedatives
- Personalized sedation and anaesthesia strategy for a given patient and ensuring all staff members know of the strategy
- Allowing adequate time for sedatives to act
- Optimal use of local anesthesia (Infiltration technqiue, volume and time to act)
- Surgical precision and technique to minimize pain