Are venograms essential? How to incoprorate venography to the venous access workflow in cardiac pacing
Role of Venography
Role of Venography
A venogram of the upper limb venous drainage at the thoraic inlet helps to delineate venous anatomy and helps guide the access method. It also helps prepare against surprises such as venous obstructions or anomalies.
A venogram entails injecting contrast material to an ipsliateral forearm vein and recording its flow proximally via fluoroscopy. About 10 ml of contrast media diluted in normal saline to fill a 20 cc syringe is used to opacify the vein. Its injection is followed by a flush of saline to clear the vein of contrast as contrast is an irritant (especially if hyperosmolar types are used). Diluted contrast is sufficient as fine details of the vein are unnecessary – only a rough outline of the veins are necessary. In modern systems, fluoroscopic recording (fluro-grab) is sufficient at 3- 5 fps with moderate level of exposure. Cine imaging is not necessary. Also note that all recordings are done in AP view. Once a venogram has been done and the vessel is noted to be patent, the operator should strive to achieve the puncture as far as possible from the clavicle (i.e. the extra-thoracic approach) as the vein is now clearly visible and that fact should be made use of.
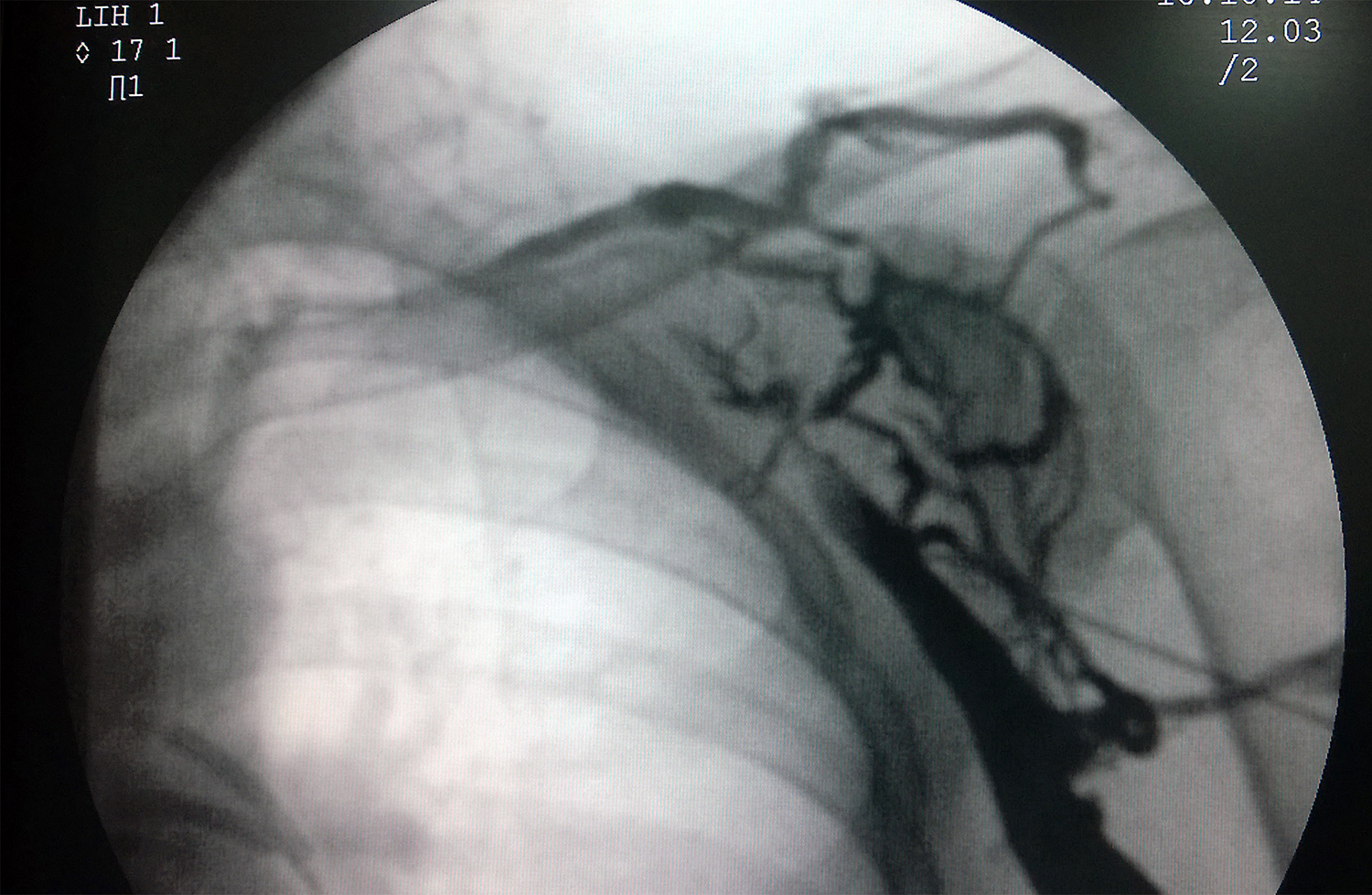
Video: The venogram does not need to be a thick stream of contrast. Small amount (5 – 10 ml) of contrast (in a contrast cocktail as described below) is more than sufficient. It is essential to cover the proximal drainage – otherwise left SVC might be missed.
Video: Too little contrast may also be problematic – but before repeating it – careful observation will ensure that you won’t miss anything. In this case (discussed elsewhere), there is a left SVC but it’s subtle.
(Note : An important observation in both above venograms is to note is that the axillary vein is seen ascending long the lateral border of the upper thoracic cage and crossing the rib margin medially at point marked by the confluence of the lateral margins of the second and third ribs. This anatomic reference is of practical value in doing an axillary vein puncture without venography)
Examples of Venous Anomalies detected by Venography

When to do a venogram ?
Some operators routinely perform venograms before puncture – in fact even before draping the site. One advantage is that the pocket can be created before the puncture and puncture can be done from the pocket itself as one is sure about the venous anatomy. The other advantage is that once the vein has been visualized, the operator can easily decide on the target entry point – well away from the clavicle – to avoid lead compression. However, although injected volumes are low, because of risks – contrast allergy and renal toxicity, routine use of venography for each and every case may be an overkill. Furthermore for simple pacing, if the operator is using fluroscopic guidance to do the vascular puncture, then extra information from the venogram may be redundant.
A more judicious use is appropriate and therefore situations where a pre-procedure venogram is helpful is given below:
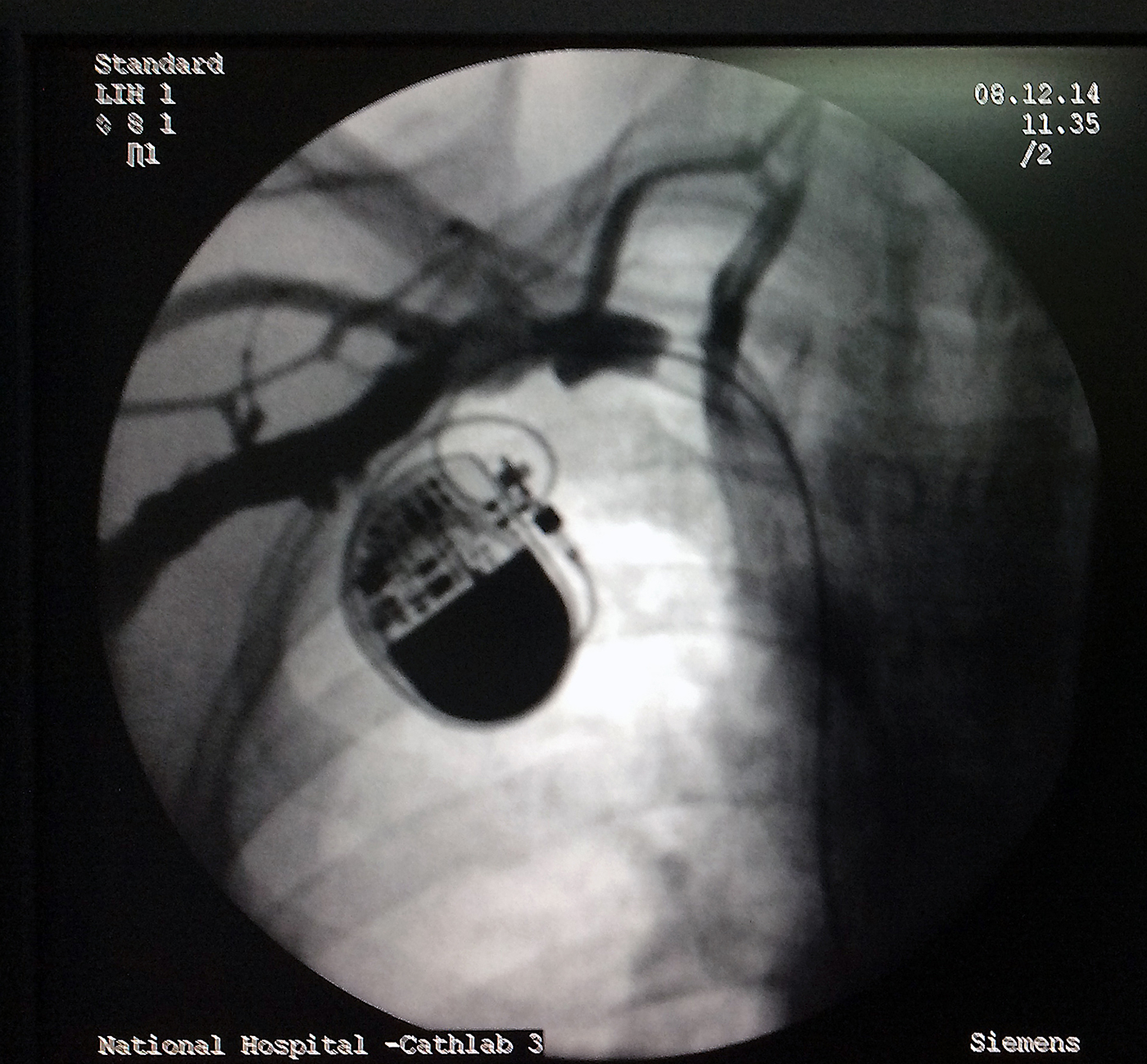
- Where pre-existing leads are present : To confirm vessel patency and guide puncture to avoid lead damage (for example when upgrading a single chamber system to a dual chamber system). This is a mandatory indication for venography
- In the grossly obese : where surface landmarks are not palpable or clearly visible
- When the risk of Pneumothorax or bleeding is high : Eg. in COPD / frail / advanced age / on anticoagulants or dual antiplatelets where a difficult puncture would lead to a penumothorax or an inadvertent arterial puncture leading to troublesome bleeding. In elderly, the vein may be significantly displaced caudally from the usual site.
- Where suspicion of a venous or anatomic deformity exists : When such arises from clinical history or examination (e.g. following ipsilateral thoracic or breast surgery or history of clavicular fracture)
- When implanting complex devices: Devices such as CRTs (Cardiac Re-synchronization Therapy) have multiple leads and need to placed friction free with adequate inter-lead spacing
Unrecognized but potentially present problem is venous spasm after venography – although the vein looks large on the fluoroscope – by the time the needle puncture is attempted, the vein would have collapsed under spasm and the operator would not know it – if this is suspected, a slow, diluted injection of 50 micrograms of GTN can relieve the spasm.